I get asked about blue light quite a lot.
“Isn’t blue light bad?”
“If it’s not harmful, then why not just use all three wavelengths; red, near-infrared, and blue at the same time?”
While red and near-infrared (NIR) light are celebrated for their ability to energise cells and promote healing, blue light plays a very different role. And yet, it’s often misunderstood, bundled into light therapy treatments with little thought to its distinct mechanism or purpose.
Here’s the thing: blue light doesn’t heal. It cleanses. It destroys. And when used appropriately, it’s an incredibly effective tool especially for surface-level conditions like acne and bacterial infections. But when misused, it can work against the very regenerative effects you’re trying to achieve with red or NIR.
In this article, we’ll break down exactly how blue light works, why it’s so different from the red end of the spectrum, and when (and when not) to use it. Because understanding the underlying mechanisms is essential to effective treatment.
Blue Light on the Spectrum: Energy, Wavelength, and Why It Matters
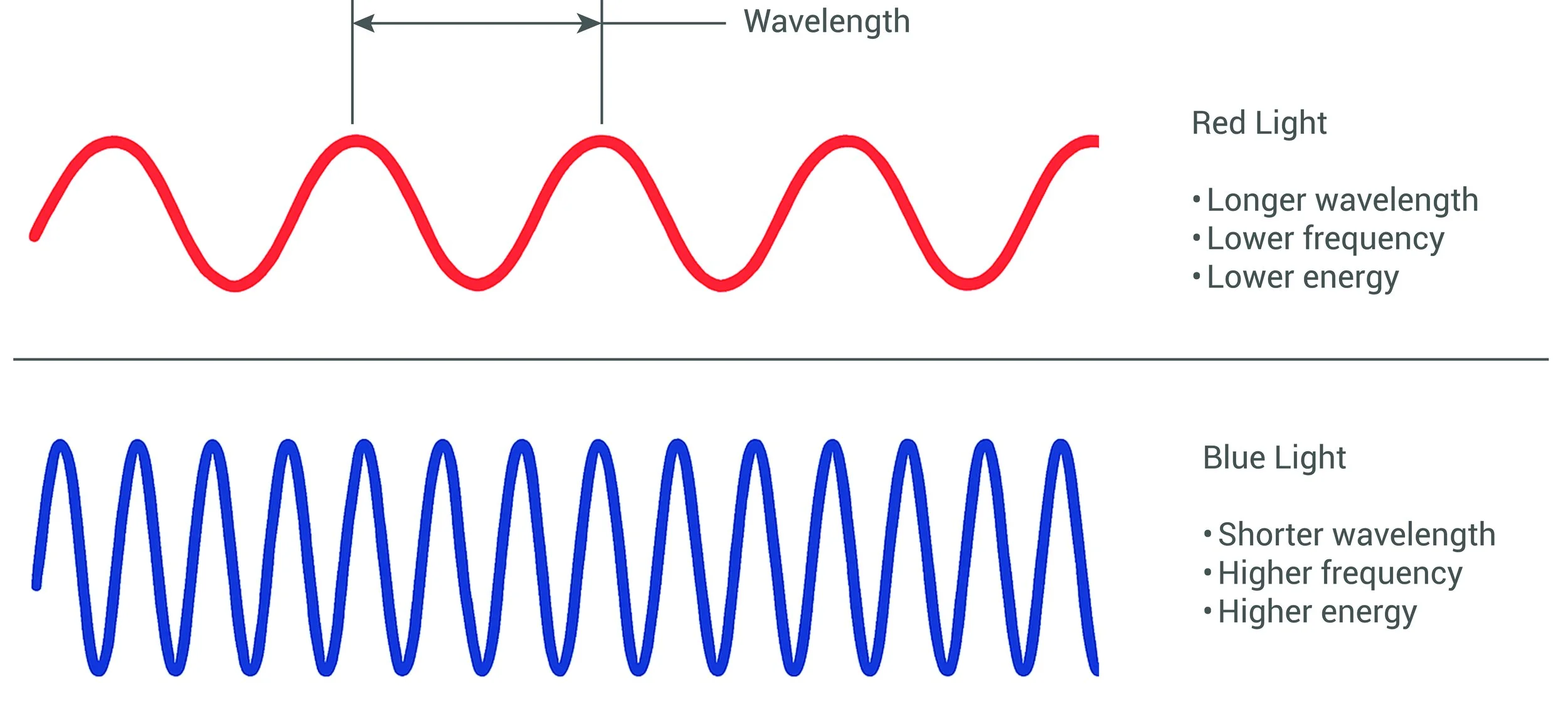
Blue and violet light occupy the lower end of the visible spectrum, spanning approximately 380 to 500 nanometres. Sitting right next to ultraviolet (UV) light on the electromagnetic spectrum, it shares some of UV’s energetic qualities but with an important distinction: it remains firmly within the visible, non-ionising range, meaning it does not carry the same DNA-damaging risks associated with UV exposure.
The only difference between UV and visible light is wavelength and frequency which together determine photon energy. As wavelengths get shorter and frequencies increase, the energy of each photon rises. That’s why UV light, with its extremely short wavelengths, can ionise atoms and damage cells. Blue light, sitting just above this threshold, still carries significant energy but without the ionising danger.
This energy becomes especially relevant in the High Energy Visible (HEV) range, typically defined as 400–450nm. HEV blue light behaves quite differently from the longer, lower-energy red and near-infrared (NIR) wavelengths used in regenerative therapy.
Because of its shorter wavelength, blue light:
Scatters more readily, limiting its depth of penetration into the skin
Primarily interacts with the epidermis and upper dermis
Is ideally suited for surface-level treatments, particularly for targeting bacteria
This makes it highly effective for antimicrobial applications. Much like UV sterilisation, blue light can disrupt and break down bacteria at the surface but crucially, it does so without the risks of ionising radiation. That’s why it has become a trusted tool in dermatology and wound care, especially in the treatment of acne and superficial infections.
In contrast, red and NIR light (typically 620 to 950+nm) operate in a completely different way. Their longer wavelengths carry less photon energy, but can penetrate much more deeply into the tissue making them ideal for deeper, cellular restorative work.
In short: blue light destructive; red light constructive. Both are powerful tools, but they serve entirely different therapeutic purposes and understanding that distinction is key to using them effectively.
Different Wavelengths, Different Outcomes: 415nm, 460nm, and 479nm
‘Blue light’ is a spectrum of wavelengths, each with unique peak effects on the body. The differences between them can be subtle in nanometres, but profound in application and outcomes. Here’s a closer look at the key wavelengths used or studied in phototherapy.
415nm – Targeted Antibacterial Action
415 nanometres is the most well-established blue light wavelength in dermatology, with a substantial body of clinical literature supporting its use, particularly for treating acne vulgaris. Sitting at the higher-energy end of the visible spectrum, it falls within the High Energy Visible (HEV) light range.
At this wavelength, photon energy is high enough to disrupt bacterial DNA, leading to a breakdown of harmful bacteria on the skin’s surface. This makes 415nm highly effective for cleansing acne-prone skin and also useful in the early stages of wound care, where reducing bacterial load is critical to preventing infection and supporting healing.
460nm – Jaundice and System Use Cases
Further up the spectrum, 460 nanometres is best known for its use in neonatal jaundice treatment. Although 460nm carries less energy than 415nm, it is still biologically active and demonstrates how blue light can influence internal metabolic processes under the right conditions. In dermatology and aesthetics, however, its topical applications are limited, it is not commonly used for antibacterial or rejuvenation protocols.
479nm – Circadian Signalling
479 nanometres marks the peak wavelength for melanopsin activation in the retina, the non-visual light receptors that regulate our circadian rhythm. Even though this part of the spectrum carries less energy per photon than the lower blue wavelengths, it’s biologically potent when it comes to signalling alertness, wakefulness, and hormonal timing.
This wavelength doesn’t play a direct role in skin therapy, but it's critically important for understanding how different wavelengths affect different systems. In this case, retinal exposure to 479nm light tells the brain that it's daytime, influencing everything from mood to metabolism.
How to Use Blue Light (and Why More Isn’t Always Better)
I get asked the following question quite a lot:
“If red, near-infrared, and blue light all do something useful, why not just use them all at once?”
It is logical, but the reality is more complex. While red and near-infrared (NIR) light are constructive, stimulating mitochondrial activity, improving cellular energy, and promoting tissue regeneration, blue light works through disruption. Its strength lies in cleansing, not repairing.
Blue Light Can Suppress Mitochondrial Function
Research suggests that short-wavelength blue light, particularly in the HEV range, can inhibit mitochondrial respiration. In simple terms, it may slow down the very healing processes that red and NIR light are designed to support.
This is why combining all three wavelengths indiscriminately, especially during a treatment aimed at rejuvenation, inflammation or healing can be counterproductive. Blue light doesn’t complement red and NIR in these contexts; it can actually undermine their regenerative benefits.
Use Blue Light Sparingly, and for the Right Reasons
Blue light is best reserved for short, controlled applications with a clear antibacterial objective such as managing acne, reducing superficial bacterial load, or supporting the initial phase of wound care. In these cases, blue light’s superficial penetration and high photon energy make it extremely effective.
Outside of these uses, applying blue light offers limited benefit and may place unnecessary oxidative stress on the skin particularly if used excessively or without a clear therapeutic rationale.
When Red and NIR Do Belong in a Blue Light Protocol
That said, there is a place for combining red or NIR with blue light but the intent matters. If the primary goal is bacterial control, then introducing red or NIR wavelengths alongside blue can help mitigate the collateral oxidative stress and support tissue recovery during or after the cleansing phase.
In other words, red and NIR can balance out a blue-light protocol but they should not be the main focus in those scenarios. The reverse is also true: if the goal is regeneration, omit blue light altogether to avoid compromising results.

Conclusion: Blue Light Is Powerful But Purposeful
Blue light is often misunderstood. It’s not inherently harmful, nor is it universally beneficial. It’s a targeted tool, and its value lies in knowing when and why to use it.
Unlike red and near-infrared light, which are restorative, blue light is disruptive and inherently has consequences/side effects.
Unlike red and near-infrared (NIR) light, which support healing and regeneration, blue light breaks down and clears. It’s highly effective for bacterial control and surface-level cleansing, but it can also inhibit mitochondrial function and introduce oxidative stress if used inappropriately.
That’s why blue light should be used sparingly and strategically, with a clear clinical purpose. In bacterial protocols, combining it with red or NIR can help buffer the side effects but if rejuvenation is the goal, omit blue entirely.
Red and NIR = Constructive
Blue = Destructive
Both are valuable but only when used with clarity and purpose.
References:
Papageorgiou, P., Katsambas, A., & Chu, A. (2000). Phototherapy with blue (415 nm) and red (660 nm) light in the treatment of acne vulgaris. British Journal of Dermatology, 142(5), 973–978.
Kawada, A., Shiraishi, H., Noda, Y., & Hiruma, M. (2002). Treatment of acne vulgaris by blue-violet light (405–420 nm) irradiation. The Journal of Dermatology, 29(11), 620–626.
Bacci, S., Bani, D., Berini, C., & De Felice, C. (2020). Blue LED light affects mitochondria and modulates reactive oxygen species: preliminary in vitro results. Lasers in Medical Science, 35(3), 603–609.
Godley, B. F., Shamsi, F. A., Liang, F. Q., Jarrett, S. G., Davies, S., & Boulton, M. (2005). Blue light induces mitochondrial DNA damage and free radical production in epithelial cells. Journal of Biological Chemistry, 280(22), 21061–21066.
Lee, M., Hwang, Y. S., & Kim, S. Y. (2020). Blue light exposure reduces mitochondrial function and viability in human keratinocytes. Journal of Photochemistry and Photobiology B: Biology, 205, 111836.